
Does your child turn their feet inwards when he walks and does this cause him to trip more? Do you get questioned a lot from neighbors, teachers, and strangers on the street: “Why does your child walk funny?” Should you be worried? Let me reassure you – this ˝funny˝ walk is called intoeing and is often seen in typically developing children and rarely persist into adolescence. If you want to know more about it, how you can help as a parent and when to visit a specialist at all, read the article below.
TL;DR – the highlights:
- intoeing gait is very common in young children – it’s part of normal development
- it should spontaneously improve by the age of 8-10 years
- shoe modifications and foot orthoses are not effective and not necessary
- encourage active play and activities that promote trunk stability
- consult your child’s doctor if intoeing is severe, and doesn’t improve with time
What is intoeing?
Some children’s feet turn inward when they walk, instead of pointing straight ahead. This is called intoeing or ‘pigeon toe’ and is very common in young children – it’s part of growing up. It’s one of the most common normal variants in children and usually occurs on both feet but can also occur on only one.
Synonyms: intoeing, in-toeing, toe-in, toeing in, pigeon toe
What problems can arise?
Children who intoe may seem to trip more often but as the child develops, the tripping becomes less frequent. However, it may be more obvious if your child has flexible joints or when they are tired. Some children may report fatigue like pain. In-toeing is part of typical development and has been shown to spontaneously resolve with age. Around 10% of children between the ages of 2 and 5 have this problem and more than 80% improve naturally with typical development.
Apart from intoeing, we can see some other compensatory mechanisms in children with increased internal rotation. These include greater step width during walking and increased ankle dorsiflexion in swing during running.1 These are normal compensation to avoid tripping. Recent findings suggest that there may be a link between increased anteversion and hip osteoarthritis in adulthood2, but it’s difficult to say with certainty that this is due to intoeing.
What causes intoeing?
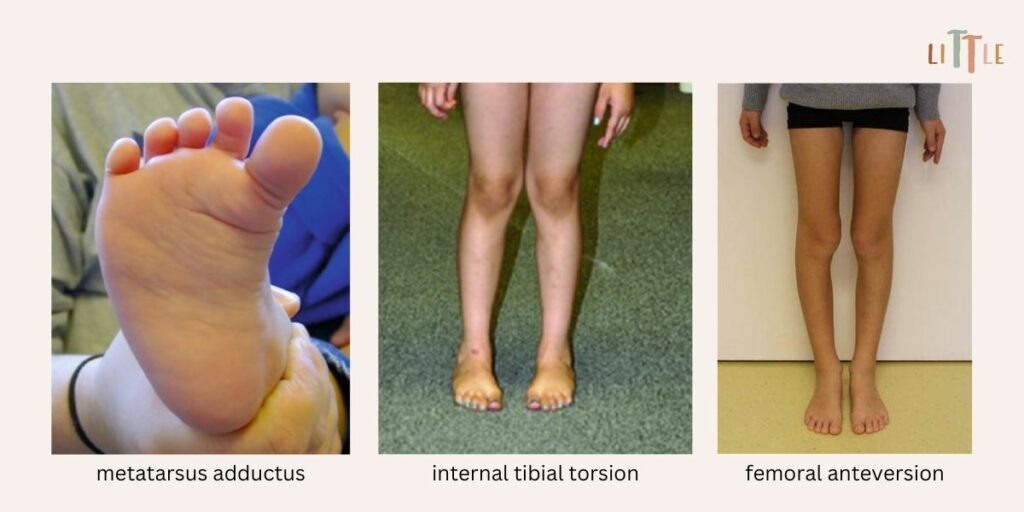
There are three main causes of in-toeing: the inward curve of the foot (metatarsus adductus), the inward turn of the lower leg (internal tibial torsion) and the inward turn of the thigh bone (femur anteversion). In each case, the rotational component is considered normal from birth to approximately 10 years of age, depending on the stage of development. Therefore, it’s important to know the normal variances and physiological development of lower leg rotation to identify abnormalities.
Metatarsus adductus: the foot is turned inwards
In this condition (sometimes called metatarsus varus) the foot curves in (C- or bean-shaped foot) with a convex lateral border of the foot. Usually, the line that bisects the heel should cross the space between the second and third toes. In children with metatarsus adductus, the line will be directed to the lateral toes. It’s often the result of a cramped space in the womb and is evident from birth. Most will resolve spontaneously but in severe cases when the foot is stiff, stretching or serial casting may be necessary.
Internal tibial torsion: inward turn of the lower leg
This occurs when the shin bone is twisted causing the foot to turn inward even though the kneecaps are facing forward. It’s most often present from 3 to 24 months of age. This usually improves by the age of 4-5 years as the bones grow, the walking pattern matures, and the knees straighten.
Femoral anteversion: thigh bone inward rotation
Intoeing can be caused by inward twisting od the bone between the hip and the knee (femoral antetorsion) and an inwrd positioning of the hip as well (femoral anteversion). These positions are normal and gradually “unwind” during development. Any delay in this normal “unwinding” gives the appearance of intoeing. In most cases this improves by the age of 5-6 years, however in some cases it may be delayed until the age of 13-14 years. It’s more common in girls than boys and can run in families.
A neurological abnormality is a completely different situation. In children with cerebral palsy, internal rotation and scissoring are common gait changes due to spasticity and hypertonia. Factors thought to contribute to the abnormal gait besides femoral antetorsion include hip-flexor tightness, imbalance of hip rotators and other hip muscle activity, and hamstring and adductor tightness as well. Apart from that, intoeing can be a symptom of other neurological conditions, such as spina bifida, congenital hip dysplasia, Blount’s disease or slipped capital femoral epiphysis. Any clinical findings such as abnormal muscle tone, gait abnormality, limitation of hip abduction, and leg length discrepancy should prompt a more intensive evaluation.
Normal growth and development of the lower limbs
In infants, the most common cause of intoeing gait is metatarsus adductus. When present in the second year of life, intoeing is usually due to internal tibial torsion. After age 3, this problem is usually due to excessive femoral anteversion.
At birth, tibial torsion is 20° to 30° internal, meaning that the ankle is internally rotated relative to the knee. During the first year of life, the angle changes, coinciding with the onset of walking, so that at 1 year of age the ankle axis should be externally rotated by approximately 10° to 12°. By age 2, tibial torsion should be about 15° to 20° external, and by age 5, it should change very little as the child reaches most of the adult norm.
Femoral anteversion at birth is around 30° to 40°. Excessive femoral anteversion usually presents as a cause of intoeing at 3 to 4 years of age. It increases until 5 to 6 years of age and then gradually decreases throughout the childhood and adolescence, finally reaching an adult value of approximately 15° to 20°.
How do we treat intoeing?
Evidence has shown that the use of nighttime bars, twister cables, or foot orthoses as well as shoe modifications are not effective in improving leg or foot position.3,4
Most children who are born with metatarsus adductus don’t need treatment. 85% to 90% of deformities identified at birth resolve without treatment by the time the child is one year old. If the child has a moderate or severe deformity that cannot be corrected passively, stretching or casting is required. Some studies suggest that moderate metatarsus adductus can improve with proper stretching during the first 8 months of life. A physical therapist should teach the parents a stretching program to ensure proper technique and to prevent overstretching of other foot structures. Severe metatarsus adductus, when the foot is stiff and cannot be manipulated, is most improved with serial casting.5,6,7
90% of excessive internal tibial torsion resolves by age 8 due to mechanical loading on the bone during upright walking activities. Braces, shoe modification or orthotics do not alter the natural course of internal tibial torsion and are not recommended. Surgery for internal tibial torsion is rarely indicated. It may be necessary in children older than 8 years with a thigh-foot angle greater than 15° of internal rotation who have severe functional impairment. The preferred option is a supramalleolar osteotomy, a surgical procedure that involves cutting the bone above the ankle to reshape or realign the bone.8
Shoe wedges, twister cables and night splints have not been shown to be effective in case of increased anteversion neither. Idiopathic altered anteversion in early childhood usually corrects on its own without interventions. Surgery is only suggested when it doesn’t improve with age and causes functional impairment, after the age of 10 and, depending on the severity, in cases of measured anteversion above 20°-50° and internal rotation higher than 80°. In these cases, femoral de-rotational osteotomy is the most effective method.9 This surgery involves cutting through the thigh bone at its upper end and turning it so that the knee is facing forwards when the child walks.
General advice – what can I do as a parent?
- It’s important for children to play and be active daily. Active play promotes bone growth and the development of motor skills.
- Encourage your child not to sit in the “W” position as it can delay or prevent the normal correction that occurs with growth and development. Instead encourage sitting cross-legged to stretch their hips in the opposite direction, but this can be more challenging.
- Out-toed activities such as ballet dancing, horseback riding, climbing, martial arts or swimming breaststroke can help improve an intoed gait that has become a habit. By encouraging these activities, the child would also work on core stabilization.
- As your child gets older, encourage walking in a straight line (keeping feet straight) to promote motor learning through task-specific training.
- There is no evidence to suggest that special shoes are beneficial, but good quality, well-fitting shoes are recommended. You should avoid buying heavy shoes as they can increase the likelihood of tripping.
- Falling is a part of the process of learning to walk and is not solely a result of intoeing.
Common misconceptions:
- my child will fail at sports – intoeing should not affect your child’s abilities to walk, run, play, participate in sports or lead a normal life
- if not treated intoeing will cause pain, increased risk of joint overloading or risk of arthritis – there is no evidence that intoeing can lead to increased joint forces during gait10, but some children may report pain
- the internal rotation muscles of the hip are tight and need to be stretched – don’t overstretch the hip into external rotation as this only cause impingement, rather encourage activities to promote core activity
| Intoeing is normal in children. However, consult your child’s doctor if: |
| • intoeing affects one side more distinctly |
| • intoeing is severe, and doesn’t improve with time |
| • intoeing causes tripping in a school-age child, which affects participation in activities |
| • the feet are stiff and don’t improve with time. |
REFERENCES:
- Byrnes SK, Kunic D, Rethwilm R, Böhm H, Horstmann T, Dussa CU. Compensatory mechanisms in children with idiopathic lower extremity internal rotational malalignment during walking and running. Gait Posture. 2020 Jun;79:46-52. doi: 10.1016/j.gaitpost.2020.03.015
- Parker EA, Meyer AM, Nasir M, Willey MC, Brown TS, Westermann RW. Abnormal Femoral Anteversion Is Associated With the Development of Hip Osteoarthritis: A Systematic Review and Meta-Analysis. Arthrosc Sports Med Rehabil. 2021 Sep 2;3(6):e2047-e2058. doi: 10.1016/j.asmr.2021.07.029
- Harris E. The intoeing child: etiology, prognosis, and current treatment options. Clin Podiatr Med Surg. 2013 Oct;30(4):531-65. doi: 10.1016/j.cpm.2013.07.002
- Uden H, Kumar S. Non-surgical management of a pediatric “intoed” gait pattern – a systematic review of the current best evidence. J Multidiscip Healthc. 2012;5:27-35. doi: 10.2147/JMDH.S28669
- Williams CM, James AM, Tran T. Metatarsus adductus: development of a non-surgical treatment pathway. J Paediatr Child Health. 2013 Sep;49(9):E428-33. doi: 10.1111/jpc.12219
- Sass P, Hassan G. Lower extremity abnormalities in children. Am Fam Physician. 2003 Aug 1;68(3):461-8. Erratum in: Am Fam Physician. 2004 Mar 1;69(5): 1049. PMID: 12924829.
- Bohne W. Metatarsus adductus. Bull N Y Acad Med. 1987 Nov;63(9):835-8. PMCID: PMC1629274
- Jones S, Khandekar S, Tolessa E. Normal Variants of the Lower Limbs in Pediatric Orthopedics. International Journal of Clinical Medicine, 2013;4(7B):12-7. doi: 10.4236/ijcm.2013.47A2004.
- Scorcelletti M, Reeves ND, Rittweger J, Ireland A. Femoral anteversion: significance and measurement. J. Anat. 2020;237: 811–26. https://doi.org/10.1111/joa.13249
- Alexander N, Brunner R, Cip J, Viehweger E, De Pieri E. Increased Femoral Anteversion Does Not Lead to Increased Joint Forces During Gait in a Cohort of Adolescent Patients. Front Bioeng Biotechnol. 2022 Jun 6;10:914990. doi: 10.3389/fbioe.2022.914990


