
As a parent, you want the best for your child. From the day they are born, you help them grow and develop in every possible way. However, did you know that the development of your child’s lower limbs is crucial to their overall health and well-being? In this article, we will explore the normal lower limb development in children and how you can help your child grow up strong.
TL;DR – the highlights:
- loading is important for healthy growth and development of the lower limbs, so it’s important to encourage children to be active
- activities with high effort (jumping, running) have a greater impact on bone growth and development than activities with low effort
- the infant’s knees are ˝bowlegged˝ but they gradually straighten as they grow
- the angulation of the knee progresses towards “knocked-knee˝ between 2 and 4 years of age
- not all children progress and develop at the same pace
- the presence of genu varus between the ages of 2 and 6 may require referral to a specialist
Understanding the importance of loading for the development of the lower limbs
As a parent, you want the best for your child and their development is one of your top priorities. One aspect of your child’s development that you may not have considered is the importance of loading on their lower limbs. Loading refers to the weight transferred to the bones, joints, and muscles of the body. During the developmental years, loading is important to promote healthy growth and development of the lower limbs. In fact, studies have shown that weight-bearing activities, such as walking and running, can have a positive effect on bone density and strength.1,2
In the early years, a child’s body grows and develops rapidly, and loading plays a key role in the formation of bones, muscles, and tissues of the lower limbs. Loading helps promote bone growth and development, strengthens muscles and tissues, and improves coordination and balance.3
Furthermore, loading is essential for proper alignment of the lower limbs.4 During normal development, the bones of the legs and feet grow and develop in a specific pattern that helps provide stability and support. Loading helps reinforce this pattern and promotes proper alignment of the lower limbs.
Does the type of load matter?
It’s important to note that not all types of loading are equal. The type of load in different situations affects the bones differently. High-impact activities such as jumping and running can help promote bone and musclegrowth, density and development2, but they also increase stress on joints and tissues. On the other hand, low-impact activities such as walking, cycling and swimming are less likely to cause injury but may not provide the same level of stimulation for growth, bone density and development.1,2
Physiologic development of lower limb alignment
The way a child’s lower limbs are aligned and positioned during weight-bearing activities has a significant impact on their overall health and well-being. During the early years of life, the lower limbs undergo a series of changes in alignment as the child grows and develops. This process is known as the physiological development of lower limb alignment.
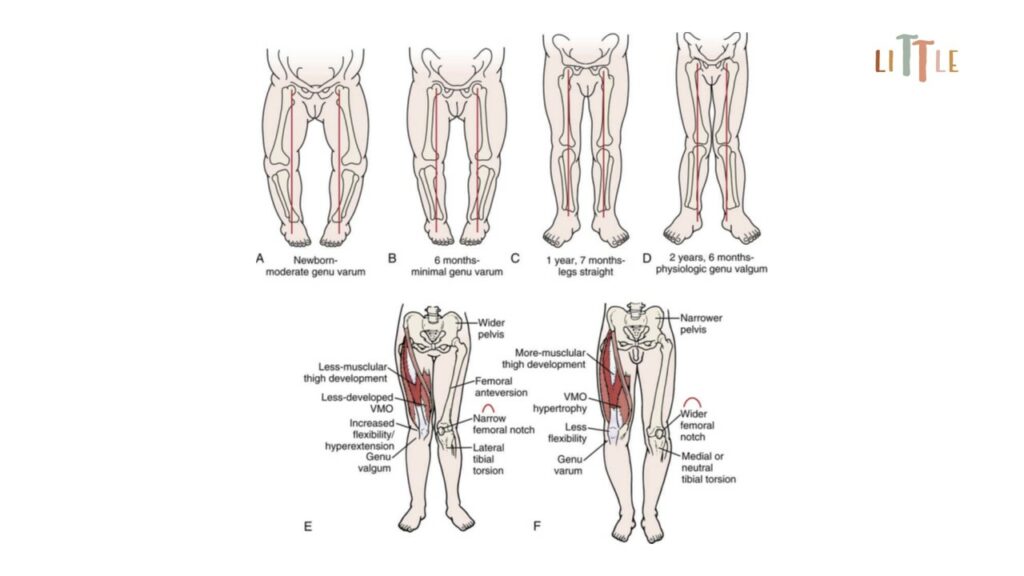
The physiological alignment of the lower limbs changes during the first years of life. Mild to moderate bowlegs in newborns and knock-knees in early childhood are a normal part of development. At birth, an infant’s knees are ˝bowlegged˝ or O-shaped (also called genu varum), but they gradually straighten until they reach a neutral alignment between the first and second year. One of the key changes that occurs during this time is progressing into a more aligned position where the knees are directly over the feet. Knee angulation then progresses towards a “knocked-knee” or X-shaped position (also called genu valgum) and reaches its peak between 2 and 4 years of age. After this time, the angle of genu valgum gradually decreases (Fig. 1).5 The final knee angle differs slightly according to race and gender. Typical values may vary, but in general, by adolescence, girls have a tibial angle between neutral alignment and slight valgum, and boys range from slight valgum to slight varum.6,7,8
However, it’s important to note that not all children progress through the physiological development of lower limb alignment at the same pace or in the same way. Some children may have conditions such as genu valgum or genu varum that affect the normal alignment of their lower limbs. In such cases, early intervention by a physical therapist can be crucial in helping the child develop normally.
When to seek professional help?
There are various opinions about when and if genu varum or valgum in young children warrants treatment. Some evidence suggests that if the varus position of the knees doesn’t decrease by the age 18 months to 2 years, bilaterally or unilaterally, further investigation is necessary, especially if the value is 25° or greater. Similarly, if the genu valgum position doesn’t decrease to the typical value of 5° to 7° but remains excessive on both sides or is present only on one side, further evaluation may be necessary.9
The pediatrician should be aware that the presence of genu varum between the ages of 2 and 6 may require referral to an orthopedic specialist. Artificially applied asymmetric compression of one epiphyseal plate of the proximal tibia with surgical stapling or tension tape can be used to correct these deformities.10
Identifying normal milestones for lower limb development
Just as children grow and develop in different ways, so does the rate at which they reach milestones in lower limb development. However, there are some general milestones that most children reach in their early years. Understanding these milestones can help parents identify potential deviations from the norm and seek early intervention if necessary.
Here are some common milestones for lower limb development:
- Crawling: Around 9 to 12 months of age, most children start crawling on their hands and knees. This is an important milestone as it helps develop the muscles and coordination of the lower limbs.
- Walking with support: Around 12 to 18 months of age, most children start walking with support. This can be by holding on to furniture or a parent’s hand. This is a key stage as it helps develop balance and coordination.
- Walking independently: Around the age of 18 to 24 months, most children take their first steps without support. At this stage, the child’s gait patterns begin to resemble those of adults, although they may still be unstable.
- Running and jumping: Around 2 to 3 years of age, most children start running and jumping. This is an important stage as it helps develop strength and coordination in the lower limbs.
It’s important to note that not all children reach these milestones at the same pace or in the same way. However, if a child consistently deviates from the norm, this may be a sign of a developmental delay or another underlying condition. In such cases, the help of a physical therapist can be crucial in the child’s development.

In conclusion, loading is an essential aspect of lower limb development, playing a key role in bone, muscle, and tissue formation and promoting proper alignment. Understanding the importance of loading and choosing activities that are appropriate for your child’s age and development is essential to helping him grow up strong. As well as understanding the physiological evolution of lower limb alignment as it helps parents understand the normal developmental process and identify possible deviations from the norm. With the help of a physical therapist, you can take proactive steps to help your child.
REFERENCES:
- Czeczelewski J, Długołęcka B, Czeczelewska E, Raczyńska B. Intakes of selected nutrients, bone mineralisation and density of adolescent female swimmers over a three-year period. Biol Sport. 2013 Mar;30(1):17-20. doi: 10.5604/20831862.1029816
- Hind K, Burrows M. Weight-bearing exercise and bone mineral accrual in children and adolescents: a review of controlled trials. Bone. 2007 Jan;40(1):14-27. doi: 10.1016/j.bone.2006.07.006
- Pax Lowes L, Hay K. Musculoskeletal Development and Adaptation. In: Campbell’s Physical Therapy for Children Expert Consult, 5th ed. Editors: Palisano R, Orlin M, Schreiber J. Elsevier, 2015; 99-116
- Ruff C, Holt B, Trinkaus E. Who’s afraid of the big bad Wolff?: “Wolff’s law” and bone functional adaptation. Am J Phys Anthropol. 2006 Apr;129(4):484-98. doi: 10.1002/ajpa.20371
- Sass P, Hassan G. Lower extremity abnormalities in children. Am Fam Physician. 2003 Aug 1;68(3):461-8. Erratum in: Am Fam Physician. 2004 Mar 1;69(5):1049. PMID: 12924829.
- Cahuzac JP, Vardon D, Sales de Gauzy J. Development of the clinical tibiofemoral angle in normal adolescents. A study of 427 normal subjects from 10 to 16 years of age. J Bone Joint Surg Br. 1995 Sep;77(5):729-32. PMID: 7559698.
- Arazi M, Oğün TC, Memik R. Normal development of the tibiofemoral angle in children: a clinical study of 590 normal subjects from 3 to 17 years of age. J Pediatr Orthop. 2001 Mar-Apr;21(2):264-7. PMID: 11242264.
- Heath CH, Staheli LT. Normal limits of knee angle in white children–genu varum and genu valgum. J Pediatr Orthop. 1993 Mar-Apr;13(2):259-62. PMID: 8459023.
- Orlin MN, Pax Lowes L. Musculoskeletal system: Structure, function, and evaluation. In: Meeting the physical therapy needs of children. 2nd ed. Editor: Effgen SK. F.A. Davis Company, Philadephia, 2013; 183-218
- Jelinek EM, Bittersohl B, Martiny F, Scharfstädt A, Krauspe R, Westhoff B. The 8-plate versus physeal stapling for temporary hemiepiphyseodesis correcting genu valgum and genu varum: a retrospective analysis of thirty five patients. Int Orthop. 2012 Mar;36(3):599-605. doi: 10.1007/s00264-011-1369-5


